What Matters Most in Psychedelic-Assisted Psychotherapy?

Marina Zlochin/AdobeStock
CLINICAL REFLECTIONS
In June, an advisory committee for the US Food and Drug Administration (FDA) recommended rejecting the psychedelic drug, midomafetamine (MDMA), as a potential treatment for posttraumatic stress disorder (PTSD). After reviewing the available data, including 2 large, randomized phase 3 clinical trials, the panel concluded that MDMA-assisted therapy was not an effective treatment and that the benefits did not outweigh the risks. While this decision is preliminary and nonbinding, it came as a shock to many in the psychedelic community, including prominent researchers, who have since published an open letter urging the FDA to reconsider the available evidence.1
One of the primary points of difference between psychedelic experts and the FDA committee relates to characterization and use of psychotherapy in the psychedelic treatment model. Researchers have long argued that psychedelics, which are given in the context of extensive preparatory and follow-up psychotherapy, act primarily as a tool to assist an innate therapeutic process. Hence the widely used term “psychedelic-assisted therapy,” or PAT, for short. However, the FDA views this characterization as confusing at best. “It is not clear,” noted the committee in their review summary, “whether the psychotherapy provided on the days of medication visits and the therapy sessions scheduled in between medication visits are necessary for the therapeutic effect of midomafetamine.”2
This is not the first time the issue of the contribution of psychotherapy to psychedelic treatment has been called into question. In July of last year, the American Journal of Psychiatry published a commentary titled “Must Psilocybin always ‘Assist Psychotherapy’?” In it, Goodwin et al argue that the characterization of psychedelics, such as psilocybin, as a psychotherapeutic intervention, as opposed to medication-based treatment, “risks confusing and impeding the development of serotonergic agonists as medications at psychedelic doses.”3 This came in the wake of the FDA publishing draft guidance for psychedelic researchers,4 which concludes similarly that “[t]he contribution of the psychotherapy component to any efficacy observed with psychedelic treatment has not been characterized.”
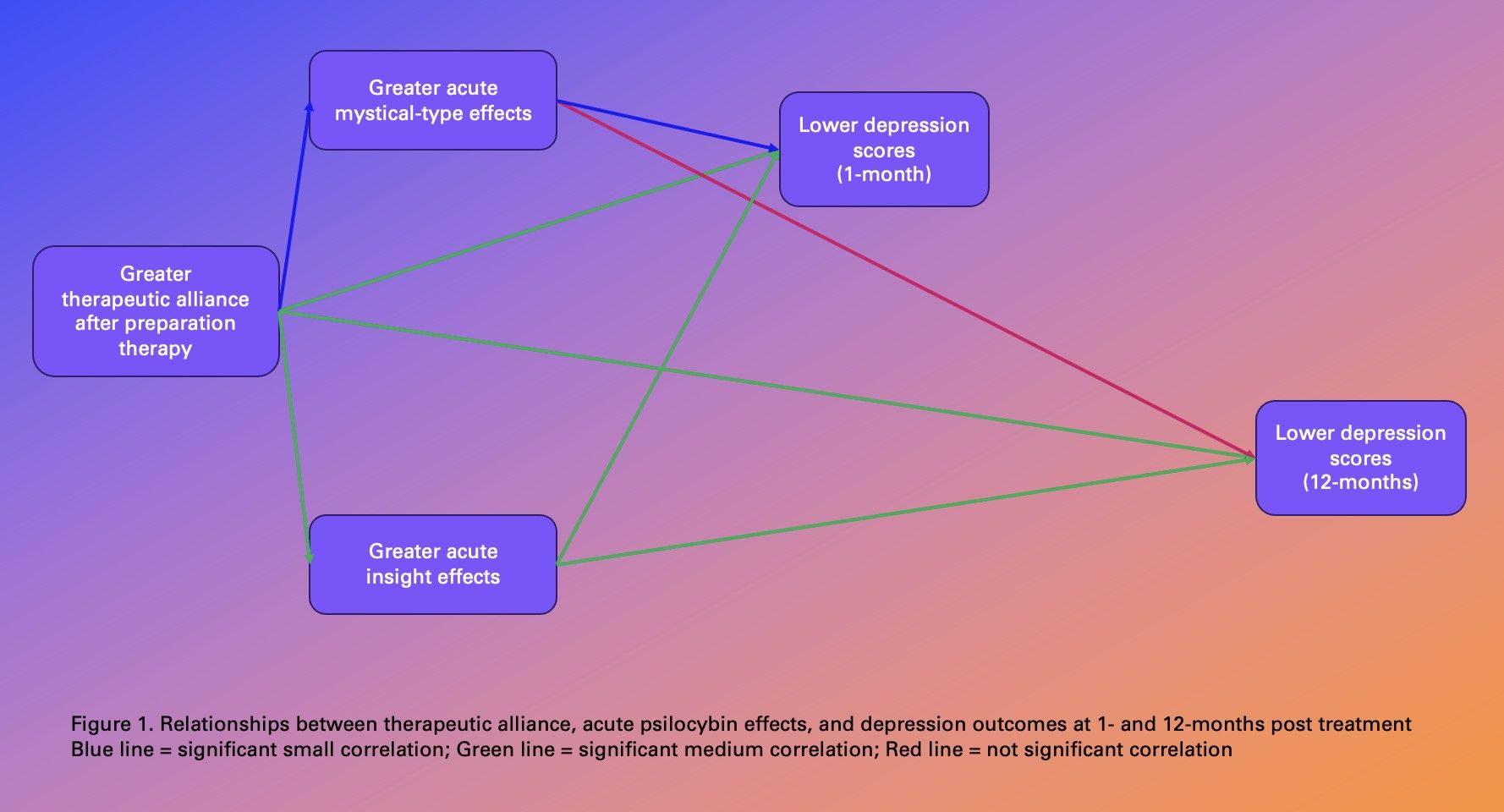
Although more data is needed to characterize the impact of psychotherapy in psychedelic treatments, there is clear evidence that the therapeutic relationship is central to their efficacy. In a randomized controlled trial of psilocybin-assisted therapy for depression at Imperial College London, the therapeutic alliance between session facilitators and participants predicted higher intensity of acute psychedelic effects, such as emotional breakthrough and mystical-type experiences, and predicted improvements in depression at long-term follow-up.5 Mirroring these findings, our team found a meaningful relationship between greater therapeutic alliance, greater intensity of acute psychedelic effects (mystical-type experiences and psychological insight), and lower intensity of depression at 1-month follow-up (see the Figure) in a randomized clinical trial of psilocybin for major depressive disorder.6 Further, the relationship between greater therapeutic alliance and lower intensity of depression persisted to 1-year after treatment, whereas the intensity of acute mystical-type effects, perhaps the most well-publicized correlate of positive response to psychedelic treatment, was not meaningfully related to depression intensity at the 1-year follow-up. This strongly suggests that the enhancement of the alliance itself is an important mechanism of action in psychedelic therapy.
Figure. Relationships between therapeutic alliance, acute psilocybin effects, and depression outcomes at 1- and 12-months posttreatment
In addition to evidence from clinical trials, there are plausible theoretical explanations for this effect. Psychedelics are known to enhance empathy and feelings of connectedness and may directly enhance relationships, including the relationship between therapists and patients. Indeed, Goodwin et al note that MDMA “notably increased empathy and sociability” and thus has “correctly, been described as assisting psychotherapy.”3 Psilocybin has also been shown to enhance empathy7,8 and feelings of connectedness, both acutely and in the weeks following drug administration.9,10 Further, psilocybin has been shown to reduce subjective and neurological responses to social exclusion,11 perhaps leading to more secure relational attachment.12 This may explain, in part, why the strength of the therapeutic alliance predicts long-term outcomes in psilocybin trials. Namely, psychedelics may unlock an innate relational capacity which is, in and of itself, healing.
This conclusion and its implications are not new to therapists or psychotherapy researchers. Decades of psychotherapy research has demonstrated time and time again that a stronger alliance is associated with positive treatment outcomes, and is a robust predictor regardless of the specific disorder, culture, or theoretical orientation.13,14 But both Goodwin et al and the FDA advisory committee seem unaware of this evidence, criticizing the PAT therapeutic model as lacking standardization and scientific rigor. Goodwin et al, for example, argue that the “relationship centered” approach espoused in PAT is the equivalent of nondirective counseling and that “there is no evidence that the conditions being targeted by psychedelics… are effectively treated by nondirective counseling.” However, based on common factors theory, all therapies are relationship centered, or should be.
“The fundamental truth of psychotherapy is this,” writes psychotherapist Jonathan Shedler. “What gets broken in a relationship must be repaired in a relationship. The relationship between patient & therapist is not incidental to therapy, it’s the active ingredient. Those who minimize it have no understanding of therapy.”15
So, where does the belief that we should minimize the role of the relationship in mental health treatment come from? This is a common tactic that has been employed by pharmaceutical and insurance companies for decades. Insurers have used exaggerated or misinterpreted findings for the efficacy of brief therapeutic interventions to justify paying for therapy only to the point of acute stabilization, typically 8 weeks, despite evidence that as many as 50% of patients require 21 sessions before sustained clinical improvement.16 Using this evidence, United Behavioral Health was recently found to have violated parity laws by refusing to pay for longer term treatments. The ruling judge described the company’s guidelines as “infected” by financial incentives, stating that “there is an excessive emphasis on addressing acute symptoms and stabilizing crises while ignoring the effective treatment of members’ underlying conditions.”17
Further, pharmaceutical companies minimize the contribution of the relationship to standard pharmaceutical treatments, such as antidepressants, whose efficacy is largely driven by nonpharmacologic factors, such as the therapeutic alliance.18 A salient example is the case of ketamine. Although evidence suggests superior efficacy of ketamine when administered in the context of psychotherapy,19,20 the pharmaceutical industry and insurance providers have promoted ketamine as a standalone drug treatment. Johnson & Johnson’s product Spravato, which is FDA approved for depression, costs thousands of dollars and is administered without any therapeutic preparation or integration therapy. Meanwhile, generic ketamine, which has proved equally efficacious and can be cheaply administered in the context of psychotherapy, is not covered by insurance.
“Health insurers have a financial incentive to steer patients to the briefest, cheapest therapies,” writes Shedler, “Executives and administrators of health care organizations are often under financial pressure to treat more patients in less time with fewer resources. All these pressures converge to turn mental health care into an assembly line. We rarely hear the voices of patients or the clinical practitioners who work with them.”21
As psychedelic research expands, participant and clinician voices are emerging, and their message is clear: the drug is only part of the story. In a trial of psilocybin for tobacco smoking cessation at Johns Hopkins, 11 of 12 participants described a deepening of their relationship with the guides as a result of the psilocybin session, and 2 participants pointed to this connection as the single most important factor in the success of their quit attempts.22
“I think if you didn’t have [the rapport] I’m not sure if it would work,” notes one participant. Another participant concludes, “It’s not just the psilocybin sessions [but] it’s that human connection, and the support that comes with that human connection, that ultimately leads to success.”
Similarly, in a depression trial at Imperial College, participants described the relationship with their guides as a “key part of the intervention” and many noted they would not use psilocybin in any other context because they “would not expose themselves to such vulnerable states of mind without experienced clinicians supporting them.”10 Further, many participants conceptualized psychedelic therapy as a long-term process and expressed the need for more follow-up: “There should be more sessions with the therapist afterwards. I needed support to incorporate it into my life.” A senior study facilitator a Johns Hopkins, Mary Cosimano, who has worked with hundreds of trial participants, has noted that themes that arise in psychedelic sessions continue well beyond long-term follow-up time points and encourages participants to seek out community based support to help with ongoing integration after the trial ends.23
Is this a new idea, or an old one? The fact that one might need extensive, specialized, support following an experience which is often rated on par with the birth of a child or death of a parent in terms of significance seems intuitive, and, indeed, for most of the history of psychedelic drug use, it has been.In many Indigenous cultures, psychedelic experiences are deeply embedded within the life of the community through extensive cosmologies, traditional rites, and social bonding.24 By comparison, the Western scientific worldview does not lend itself easily to understanding or integrating such experiences. Exemplifying the need for such support, Rachael Peterson, a current student at Harvard Divinity School and past trial participant at Johns Hopkins said that the experience “upended my understanding of ultimate reality—an upending sometimes referred to as an ‘ontological insurgency’. All I know is that for a moment, I opened to the possibility of being outside everything that matters, and the space between threw me back on myself, rendered me uncanny. Cast out, I could not find my place again in the order of things. Choking, breathless, I was having a grief-tinged cosmic panic attack.”25
Is it reasonable to conclude that a person could walk out of a session following such an experience, as if having received a vitamin infusion, Botox injection, or standard antidepressant medication, and reintegrate into the world without ongoing, human, support? Do we need a randomized controlled trial to conclude that such an experience would benefit from further therapeutic engagement?
Goodwin et al rightly argue that “any complex interaction with a therapist during the active drug experience clearly complicates interpretation of treatment outcomes…” But is it ultimately possible, or even advisable, to disentangle human interaction from any form of treatment, much less one that can result in a “cosmic panic attack”? Perhaps, rather than trying to rid psychedelic therapy trials of all human interaction in order to better isolate the effect of drug administration, thereby maximizing pharmaceutical and insurance control over who can access this treatment, we should instead acknowledge the limitations of this particular form of knowledge formation and use other means to discern best practices. Intuition, clinical judgement, and an appreciation for the thousands of years of history surrounding the use of psychedelic drugs26 could be a good start.
Dr Levin is a psychiatrist and post-doctoral scholar at the Center for Psychedelic Drug Research and Education in the Ohio State University College of Social Work. Dr Davis is an associate professor and director of the Center for Psychedelic Drug Research and Education in the College of Social Work at the Ohio State University and an adjunct professor at Johns Hopkins.
Disclosures: AKD is supported by the Center for Psychedelic Drug Research and Education at Ohio State University, funded by anonymous private donors and is supported by the Johns Hopkins Center for Psychedelic and Consciousness Research, funded by Tim Ferriss, Matt Mullenweg, Craig Nerenberg, Blake Mycoskie, and the Steven and Alexandra Cohen Foundation. AKD is President of Source Research Foundation. The clinical trial examining psilocybin-assisted therapy for people with Major Depressive Disorder was funded in part by a crowd-sourced funding campaign organized by Tim Ferriss and a grant from the Riverstyx Foundation.
References
1. Experts endorse MDMA-assisted therapy for PTSD. July 7, 2024. Accessed July 16, 2024. http://scientiststatementonptsd.com
2. Food and Drug Administration. Psychopharmacologic Drugs Advisory Committee Meeting. 2024;FDA Briefing Document. https://www.fda.gov/media/178984/download
3. Goodwin GM, Malievskaia E, Fonzo GA, Nemeroff CB. Must psilocybin always “assist psychotherapy”? Am J Psychiatry. 2024;181(1):20-25.
4. US Food and Drug Administration. Psychedelic drugs: considerations for clinical investigations; guidance for industry; draft guidance. Regulations.gov. June 26, 2023. Accessed July 10, 2024. https://www.regulations.gov/document/FDA-2023-D-1987-0002
5. Murphy R, Kettner H, Zeifman R, et al. Therapeutic alliance and rapport modulate responses to psilocybin assisted therapy for depression. Front Pharmacol. 2022;12.
6. Levin AW, Lancelotta R, Sepeda ND, et al. The therapeutic alliance between study participants and intervention facilitators is associated with acute effects and clinical outcomes in a psilocybin-assisted therapy trial for major depressive disorder. PLoS One. 202419(3):e0300501.
7. Pokorny T, Preller KH, Kometer M, et al. Effect of psilocybin on empathy and moral decision-making. Int J Neuropsychopharmacol. 2017;20(9):747-757.
8. Mason NL, Mischler E, Uthaug MV, Kuypers KPC. Sub-acute effects of psilocybin on empathy, creative thinking, and subjective well-being. J Psychoactive Drugs. 2019;51(2):123-134.
9. Kettner H, Rosas FE, Timmermann C, et al. Psychedelic communitas: intersubjective experience during psychedelic group sessions predicts enduring changes in psychological wellbeing and social connectedness. Front Pharmacol. 2021;12.
10. Watts R, Day C, Krzanowski J, et al. Patients’ accounts of increased “connectedness” and “acceptance” after psilocybin for treatment-resistant depression. J Humanist Psychol. 2017;57(5):520-564.
11. Preller KH, Pokorny T, Hock A, et al. Effects of serotonin 2A/1A receptor stimulation on social exclusion processing. Proc Natl Acad Sci U S A. 2016;113(18):5119-5124.
12. Stauffer CS, Anderson BT, Ortigo KM, Woolley J. Psilocybin-assisted group therapy and attachment: observed reduction in attachment anxiety and influences of attachment insecurity on the psilocybin experience. ACS Pharmacol Transl Sci. 2021;4(2):526-532.
13. Baier AL, Kline AC, Feeny NC. Therapeutic alliance as a mediator of change: a systematic review and evaluation of research. Clin Psychol Rev. 2020;82:101921.
14. Flückiger C, Del Re AC, Wampold BE, Horvath AO. The alliance in adult psychotherapy: a meta-analytic synthesis. Psychotherapy. 2018;55(4):316-340.
15. @JonathanShedler. The fundamental truth of psychotherapy is this: What gets broken in a relationship must be repaired in a relationship. The relationship between patient & therapist is not incidental to therapy, it’s the active ingredient. Those who minimize it have no understanding of therapy. January 8, 2021. Accessed July 10, 2024. https://twitter.com/JonathanShedler/status/1347626054156865537
16. Lambert MJ, Hansen NB, Finch AE. Patient-focused research: using patient outcome data to enhance treatment effects. J Consult Clin Psychol. 2001;69(2):159-172.
17. Abelson R. Mental health treatment denied to customers by giant insurer’s policies, judge rules. The New York Times. March 5, 2019. Accessed July 10, 2024. https://www.nytimes.com/2019/03/05/health/unitedhealth-mental-health-parity.html
18. Leuchter AF, Hunter AM, Tartter M, Cook IA. Role of pill-taking, expectation and therapeutic alliance in the placebo response in clinical trials for major depression. Br J Psychiatry. 2014;205(6):443-449.
19. Dakwar E, Anerella C, Hart CL, et al. Therapeutic infusions of ketamine: do the psychoactive effects matter? Drug Alcohol Depend. 2014;136:153-157.
20. Rothberg RL, Azhari N, Haug NA, Dakwar E. Mystical-type experiences occasioned by ketamine mediate its impact on at-risk drinking: results from a randomized, controlled trial. J Psychopharmacol. 2021;35(2):150-158.
21. Aftab A. Psychoanalysis and the re-enchantment of psychiatry: Jonathan Shedler, PhD. Psychiatric Times. July 29, 2020. https://www.psychiatrictimes.com/view/psychoanalysis-re-enchantment-psychiatry-jonathan-shedler-phd
22. Noorani T, Garcia-Romeu A, Swift TC, et al. Psychedelic therapy for smoking cessation: qualitative analysis of participant accounts. J Psychopharmacol. 2018;32(7):756-769.
23. Noorani T. Making psychedelics into medicines: the politics and paradoxes of medicalization. Journal of Psychedelic Studies. 2020;4(1):34-39.
24. Beyer SV. Singing to the Plants: A Guide to Mestizo Shamanism in the Upper Amazon. University of New Mexico Press; 2010.
25. Peterson R. A theological reckoning with ‘bad trips.’ Harvard Divinity Bulletin. Accessed July 10, 2024. https://bulletin.hds.harvard.edu/a-theological-reckoning-with-bad-trips/
26. Winkelman MJ. The evolved psychology of psychedelic set and setting: inferences regarding the roles of shamanism and entheogenic ecopsychology. Front Pharmacol. 2021;12:619890.
link

:max_bytes(150000):strip_icc()/mental-illnesses-serve-us-military-3973352_Final-8bf4b36ae7bd41188738702ac3c297c7.png "Can You Join the Military With Depression, Anxiety, or Other Mental Illness?")


:max_bytes(150000):strip_icc()/Health-GettyImages-2222718735-eccdfcbd45b04d8fa98ecdad691be69c.jpg "6 Signs Your Gut Health Is Out of Balance")


 consensus statement on the definition and scope of gut health")